
Anal Fissure Treatment and Surgery
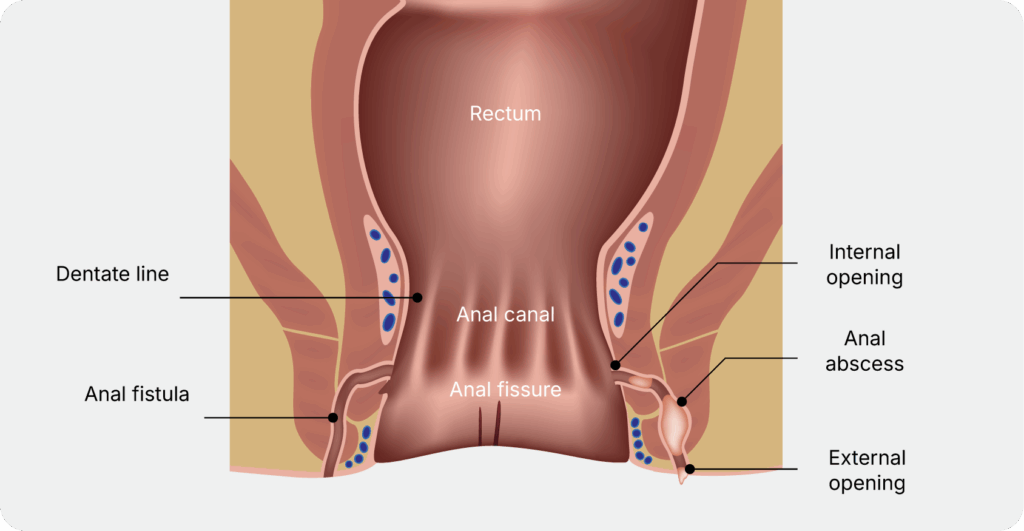
What Is an Anal Fissure?
Symptoms of an Anal Fissure
Anal fissure symptoms include pain during or after bowel movements, and bright red blood on the stool or toilet paper. Other symptoms include these:
- Sharp, tearing, or “cuttingˮ pain during bowel movements
- Burning, itching, or irritation around the anus
- Spasm or tightness of the anal sphincter
- A visible crack in the skin around the anal area
- Reluctance to pass stool due to pain, which can worsen constipation
- A small skin tag near the fissure in (more commonly seen in chronic cases)
When Should You See a Doctor?
Many fissures can improve with simple measures, but others may need medical attention. See a specialist if you experience any of the following:
- Pain or bleeding that does not improve after 1-2 weeks of self-care
- Recurrent fissures that keep coming back
- Severe pain that makes bowel movements difficult
- Bleeding that is heavy, persistent, or not clearly linked to a bowel movement
- Fissures that are painless, multiple, or located away from the typical midline position
- Fissures associated with discharge, fever, weight loss, diarrhoea, or symptoms inflammatory bowel disease
Not all anal bleeding is due to fissures. Haemorrhoids, infections, inflammatory bowel disease, polyps, and colorectal cancer can also cause similar symptoms. A professional medical evaluation is important to determine the underlying cause and rule out other possible conditions.
Consult a Specialist for Anal Fissure Treatment Options
If you have pain, bleeding, or any of the symptoms listed above, speak with our specialist for an assessment and treatment plan.
How Are Anal Fissures Diagnosed?
Non-Surgical Treatment for Anal Fissures
Non-surgical treatment is the first-line approach for most fissures, especially acute ones.
The goals are to soften stool, reduce pain, relax the anal sphincter, reduce pressure around the fissure, and promote healing of the tear.
Stool Softening and Constipation Control
- Increase fibre gradually through diet or supplements
- Drink enough water to stay well hydrated
- Use stool softeners or osmotic laxatives if needed
- Avoid straining and prolonged sitting on the toilet
- Manage diarrhoea if loose stools are contributing to irritation
Warm Sitz Baths
Pain Relief
Oral painkillers may be used when appropriate. Topical anaesthetic creams may provide short-term pain relief but should not replace treatments that promotes healing.
Topical Medications
When Is Surgery Needed for an Anal Fissure?
What to Expect
Before the Procedure
During the Procedure
Anal fissure surgery is usually performed as a day surgery under general anaesthesia or regional anaesthesia. Most patients are able to go home on the same day.
The fissure surgery procedure used will depend on your circumstances.
- Lateral Internal Sphincterotomy: This is the most commonly performed fissure surgery procedure for chronic anal fissures. The surgeon makes a small cut in part of the internal sphincter muscle to reduce resting pressure and support healing of the fissure.
- Fissurectomy: This involves removing the chronic fissure tissue and associated scar tissue or skin tag. It may be performed on its own or in combination with other techniques, and may be considered when sphincterotomy carries a higher risk of incontinence.
After the Procedure
Most patients go home the same day. Mild discomfort, bleeding, and discharge is relatively common in the early days after surgery. Pain often improves as the sphincter spasm settles.
It is important to continue stool softeners, maintain good hydration, eat adequate fibre, and take warm sitz baths if directed during recovery.
Our team will arrange follow-up appointments to monitor your healing and address any ongoing symptoms.
Recovery After Anal Fissure Treatment or Surgery
- Keep stools soft
- Avoid straining
- Clean the area gently after bowel movements
- Use warm baths if advised
- Take pain relief as prescribed
- Attend follow-up appointments
Who Is Suitable for Anal Fissure Surgery?
Anal fissure surgery is not appropriate for everyone. Suitability must be assessed on an individual basis.
Surgery may be considered for:
- Patients with chronic fissures that have not healed after appropriate medical treatment
- Patients with recurrent fissures causing repeated pain and bleeding
- Patients with high resting sphincter tone and classic posterior midline fissures (for lateral internal sphincterotomy)
- Patients with continence risk factors, where alternatives to sphincterotomy, such as botulinum toxin, fissurectomy, or advancement flap procedures, may be considered
The most appropriate treatment approach depends on a careful review of each patientʼs history, assessment findings, and individual circumstances.
Consult a Specialist for Suitable Treatment Options
Experiencing the symptoms of an anal fissure? Speak with our specialist to find the right anal fissure cure for your condition, whether non-surgical or surgical.